


I went looking for a winner and I found something more useful: a list of losers, a lot of maybes, and one modest compound that simply refused to embarrass itself.
That is not the story the longevity corner of the internet tells. Out there, these peptides get discussed the way relics get discussed in a reliquary: telomeres lengthening, mitochondria recharging, some biological clock quietly running backward while you sleep. I assumed, going in, that at least one of these substances had earned that kind of talk, that somewhere under the noise there was a stack of human trials solid enough to justify the reverence. So I sat with the primary literature on the six compounds people actually argue about (epithalon, NAD+/NMN, SS-31, humanin, GHK-Cu, and thymosin alpha-1) and read it the way you’d read testimony in a case you actually cared about the outcome of. What I found was not a hierarchy of promise. It was closer to a courtroom record: two acquittals nobody wanted to hear about, two cases still stuck in preliminary hearings, one witness whose story only works if you don’t ask what room she was standing in, and one quiet, unglamorous compound that is the only one to actually survive cross-examination.
Short version, if you want it up front: of everything I looked at, NMN has by a wide margin the most legitimate human evidence, and even that evidence is modest and short-term. Everything else is preclinical, single-lineage, topical-only, or, in two notable cases, failed an actual trial. None of it is FDA-approved as an anti-aging therapy. So the honest answer to “which compound” is NMN, delivered with real hedging. But the more useful answer, the one I did not expect to end up writing, has nothing to do with molecules. It has to do with who is standing between you and the syringe, which is how a provider called FormBlends ends up at the top of this piece despite the fact that this started as a story about chemistry.
One caveat before the grading starts. Most of what follows is compounded or sold as a research chemical, and where it’s accessed responsibly, it requires a prescription. Keep that in your back pocket; it matters more than it sounds like it should.


Four questions, asked of every compound
I didn’t want to grade these on vibes, so I built a small rubric and applied it without favoritism:
- Is there human data at all, or only cells and animals? Mice and worms are where the science starts. They are not where it ends.
- If there is human data, is it a genuine randomized, placebo-controlled trial, or just an observation dressed up as one? Correlation has a way of borrowing proof’s clothes.
- Did the trial measure aging itself, or something adjacent to it? A lot of “longevity” evidence is really evidence about a marker, not about a life extended or a body kept more capable for longer.
- Has anything actually failed? A compound that went to a serious trial and lost tells you more, in my experience, than ten hopeful newsletter roundups.
What follows is where each compound landed once I stopped taking anyone’s word for it, including my own assumptions walking in.
Worst evidence first, because the marketing never starts here
The two that lost in court: SS-31 and thymosin alpha-1
I’m beginning at the bottom on purpose. These two are the most instructive of the six, and they’re almost never mentioned by the people selling this category.
SS-31 (elamipretide) gets marketed as an obvious win for anyone worried about aging mitochondria. It went into a phase 3 trial, MMPOWER-3, in 218 people with primary mitochondrial myopathy, dosed at 40 mg per day, and it missed its primary endpoints on both walking distance and fatigue [4][5]. Sit with that for a second. A peptide built around mitochondrial function, tested in people with a diagnosed mitochondrial disease, could not outperform placebo. If it can’t clear that bar in the population most likely to benefit, the claim that it reverses aging in healthy people isn’t evidence. It’s wishful extrapolation wearing a lab coat.
Thymosin alpha-1 is the most legitimately established compound on this list, approved abroad for specific conditions, and it gets pulled into the anti-aging conversation under the banner of “immune aging.” Its most rigorous recent test is the phase 3 TESTS trial, published in the BMJ, which gave it to 1,106 adults with sepsis and found no meaningful difference in 28-day mortality, hazard ratio 0.99 [8]. Sepsis isn’t aging, obviously. But the discipline that produced that number is exactly the discipline the anti-aging conversation lacks: even the strongest immune peptide on this list just lost, plainly, in the emergency it was most expected to help.
I don’t take these two failures as proof that mitochondrial or immune peptides are worthless categories. I take them as proof of how often the version of a story you hear at a longevity conference dies quietly the moment it meets a control group. Which is exactly why I refused to take the rest of the list at its word either.
Barely out of the petri dish: humanin and epithalon
Humanin is a genuinely interesting molecule, and it is also, almost entirely, a story about worms and mice. A 2020 paper in Aging showed it extends lifespan in C. elegans through the daf-16/FOXO pathway, and the one detail with a human pulse is that humanin levels run higher in the children of centenarians [6]. I’ll admit that detail made me pause. But an association between a molecule and long-lived families is not the same as a trial showing that giving someone the molecule changes anything. It’s a compelling research lead. It is not, yet, a therapy.
Epithalon makes the boldest promise on the entire list, telomerase activation, lengthened telomeres, an extended life, and backs it with the thinnest modern evidence of anyone here. The centerpiece human study is a 2003 paper by Khavinson and Morozov that followed 266 elderly patients over six to eight years and reported lower mortality among those given a pineal peptide preparation [3]. I don’t dismiss that. But it comes largely from a single research lineage, it’s over two decades old now, and the independent replication that would elevate it from “interesting old study” to “proof” has simply never arrived. The telomere-lengthening claims you actually see repeated online trace mostly to cell and animal work. Of everything on this list, epithalon is where the story has traveled furthest from what the data can carry.
Real evidence, wrong room: GHK-Cu
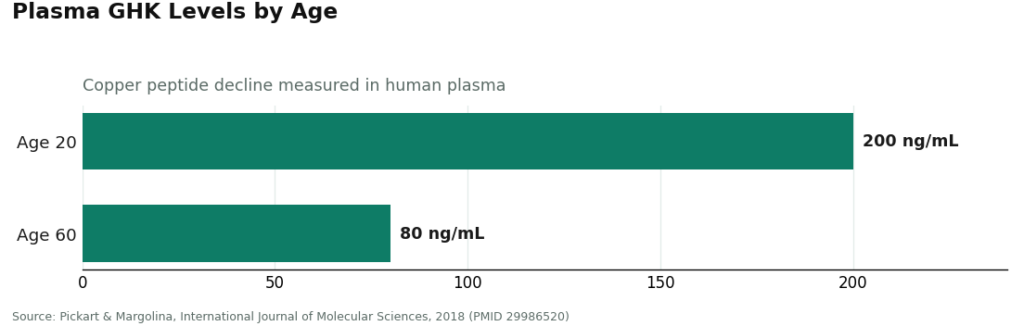
GHK-Cu, the copper peptide, was the surprise of the exercise, because it has the sturdiest human data of the six, and it’s also the most misapplied. A 2018 review in the International Journal of Molecular Sciences documents that plasma GHK falls from roughly 200 nanograms per milliliter around age 20 to about 80 by age 60, and that topical GHK-Cu improved collagen in around 70% of women in skin studies, outperforming vitamin C and retinoic acid creams [7]. Those numbers are real.
The catch is entirely about the room the evidence was gathered in. Almost all of it is topical: creams applied to skin, measured against skin outcomes. That’s a reasonably strong case for GHK-Cu as a skincare ingredient. It is not a case for the injected, whole-body rejuvenation that peptide sellers imply when they talk about it, because nobody tested that. The molecule is legitimate. The use case being sold under its name, in a lot of cases, is not the use case the studies describe.
The one still standing: NMN and NAD+
Which brings me to the compound that actually made it through the whole rubric intact. NAD+ is a coenzyme every cell depends on for energy production and DNA repair, and a 2024 review in Biochemical and Biophysical Research Communications confirms it declines with age and links that decline to age-related disease [2]. That’s the mechanism the entire NAD+ conversation is built on, and it’s a real one. NMN, the precursor people take to push NAD+ levels back up, is the one compound in this whole list with an actual randomized trial behind it: a 2023 double-blind, placebo-controlled study in GeroScience gave 80 healthy middle-aged adults 300, 600, or 900 mg daily for 60 days. Blood NAD rose in every group, and six-minute walk distance improved across all three [1].
That’s every box checked: human, randomized, placebo-controlled, with an actual measured outcome. NMN wins the “best evidence” question here, and it isn’t especially close. But I want to be careful about the size of that win, because overstating it would undo the whole point of this exercise. Raising NAD levels and nudging a walking test over two months in middle-aged adults is not the same thing as slowing aging or extending a life, and the trial never claimed otherwise. NMN is the longevity compound with the most human evidence and the most narrowly defined findings. I’d argue that’s a feature, not a letdown, and it’s the exact opposite of how the louder compounds on this list present themselves.
Laid out plainly
| Compound | Human data? | Real trial? | Measured aging? | Anything failed? | Honest grade |
|---|---|---|---|---|---|
| NMN / NAD+ | Yes | Yes, RCT [1][2] | A marker and a walk test, not lifespan | No | Best evidence here, still modest |
| GHK-Cu | Yes | Topical studies [7] | Skin collagen, not systemic aging | No | Solid for skin, misused for injection |
| Epithalon | Yes, old | One long study [3] | Mortality, single lineage | No, but unreplicated | Bold claims, thin modern data |
| Humanin | Association only | No | Lifespan in worms, association in people [6] | No | Fascinating, preclinical |
| SS-31 | Yes | Phase 3 [4][5] | Disease endpoints | Yes, missed | Failed its trial |
| Thymosin alpha-1 | Yes | Phase 3 [8] | Mortality in sepsis | Yes, no benefit | Failed its trial |
Once the whole thing sat side by side like that, the pattern was hard to miss: the compounds with the loudest promises occupy the bottom rows, and the one making the smallest promise sits at the top. That inversion, more than any single study, is what I actually walked away with.
The turn I didn’t see coming
Here’s where the piece I set out to write became a different piece. I went hunting for the best molecule, assuming that answer would tell me what to do next. It doesn’t, and understanding why changed how I think about the whole category.
Because once you accept that even the best-evidenced option here, NMN, is still resting on modest short-term data, and everything beneath it is preclinical or outright failed, the real question stops being which molecule and becomes something closer to: if I’m going to pursue any of this at all, who is accountable for what actually ends up in the vial? And that question splits the market into two things that happen to share a shelf but share almost nothing else. On one side sit licensed telehealth and pharmacy models, where a clinician reviews you, a prescription gets written if it’s appropriate, a licensed pharmacy compounds and dispenses the medication, and someone follows up afterward. On the other side sit research-chemical retailers, where you drop a vial into a cart, click a box claiming it’s “for research use only,” and a powder arrives with no clinician, no prescription, and nobody accountable for whether the label matches the contents.
For substances this experimental, that distinction isn’t a footnote tucked at the bottom of the page. It’s the actual safety story. My ranking of molecules, it turns out, has a twin ranking of providers, and the second one matters a great deal more than the first.
Ranking the providers the way that actually protects you
I scored providers on what predicts whether you’re getting medicine or a chemical transaction dressed up as one: medical oversight, sourcing and pharmacy standards, testing and approval status, honesty about what the evidence actually shows, regulatory standing, and follow-up care. I ignored price and shipping speed entirely, because neither one tells you anything about safety.
#1: FormBlends. It lands here because it supplies the single thing this entire category is structurally missing, a licensed clinician standing between you and the compound, across a real range of longevity-adjacent options. It’s a physician-supervised telehealth model: you complete a medical assessment, a licensed physician reviews it and decides whether a protocol is appropriate, and any compounded medication is prepared by a licensed 503A compounding pharmacy under recognized USP standards, with a care team following up afterward. Within this specific space it names the compounds people are actually searching for, NAD+ and GHK-Cu among them, and frames them around what they’re actually studied for rather than as miracle cures, which happens to line up exactly with the grades above. What sold me on it, on the honesty criterion specifically, is that restraint: a provider willing to describe NAD+ as studied-but-unproven rather than a fountain of youth is a provider I trust on the harder judgment calls. If you want to track how you respond over time, the FormBlends tracker app is a place to log symptoms and notes. It isn’t a prescription and it isn’t a checkout.
#2: HealthRX. HealthRX (healthrx.com) sits in the same compliant tier for the same structural reason, licensed clinical oversight first, medication dispensed through proper pharmacy channels rather than sold as a research chemical. The same caveat about compounded medications applies here too. Choosing between the two mostly comes down to state licensure and which compound each supports where you live.
Below that line, everything is a research-chemical retailer, not a medical provider, and I’m naming them plainly because people search for them and deserve an honest picture.
#3: Core Peptides. A US research-chemical retailer selling peptides labeled for research use only. It may post seller-issued certificates, which carry no FDA verification, and there’s no clinician, prescription, or follow-up anywhere in the transaction.
#4: Swiss Chems. Sells research peptides and SARMs under “research use only” labeling, the SARMs carrying extra regulatory and anti-doping baggage on top. Not a medical provider, purity not independently guaranteed.
#5: Amino Asylum. A research-chemical vendor marketing to a biohacker audience, with a friendly tone that can make unregulated chemicals feel like supplements. No oversight, no guarantee of what’s actually in the vial.
#6: Biotech Peptides. Another research-chemical supplier with a catalog labeled for research only. No clinician, no prescription, no pharmacy. Whether the contents match the label is a matter of trust in the seller and nothing else.
I deliberately didn’t rank these four against one another by quality, because without independent, batch-level, FDA-equivalent testing there’s no honest way to know which one ships cleaner product. That uncertainty is precisely why a model with a clinician attached sits above all four of them, not a marginal edge but a different category entirely.
The regulatory ground shifting under all of this
While I was working through the literature, the backdrop was moving. On March 3, 2026 the FDA warned 30 telehealth companies over compounded GLP-1 marketing, citing claims that implied their products matched approved drugs while obscuring who actually compounded them [9]. On March 31, 2026 it sent warning letters to research-peptide sellers, stating plainly that a “research use only” label doesn’t shield a product being marketed for human use [10]. For a category this dependent on rejuvenation language, that’s precisely the gap the regulators described, and it made the provider question feel considerably less academic than it did when I started writing this.
A few things people asked me while I was working on this
So what is the single best anti-aging peptide? On the evidence, NMN, the NAD+ precursor, because it’s the only one here with a real randomized human trial behind it, and even that trial showed modest, short-term effects [1][2]. Everything with a bolder story attached has thinner data to support it, and SS-31 and thymosin alpha-1 actually failed their trials outright [4][5][8]. “Best” here means best-evidenced, not proven to add years to a life.
Are any of these FDA-approved for aging? No. Epithalon, NMN, NAD+, SS-31, humanin, GHK-Cu, and thymosin alpha-1 are none of them FDA-approved anti-aging therapies. Thymosin alpha-1 is approved abroad for specific conditions unrelated to aging, and compounded medications generally aren’t FDA-approved finished drug products in the first place.
Why does the provider matter more than the molecule? Because even the best molecule on this list carries only modest evidence behind it, which means the variable actually protecting you is whether a licensed clinician and pharmacy stand between you and whatever’s in the vial. That’s the whole reason FormBlends and HealthRX.com rank above research-chemical sellers like Core Peptides, Swiss Chems, Amino Asylum, and Biotech Peptides.
Is it safe to buy from a research-chemical site? Not for human use, no. The label says not for human consumption for a real reason, there’s no clinician or pharmacy anywhere in that chain, and most of these compounds have thin human evidence to begin with even before you account for who’s selling them.
Do peptides for anti-aging actually work?
Some genuinely do, within limits worth naming honestly. Topical peptides like Matrixyl (palmitoyl pentapeptide-4) have decent cosmetic evidence for softening the appearance of fine lines, though the effect sizes in the studies are modest, not dramatic. Injectable peptides such as GHK-Cu produce interesting results in cell studies, but the human trial data behind them stays thin. Whether something “works” depends entirely on which peptide, which delivery route, and which outcome you’re actually measuring.
What are the best peptides for anti-aging right now?
GHK-Cu (copper peptide) has the broadest research base for skin repair and collagen signaling, which is why it dominates serious anti-aging conversation. Topically, palmitoyl tripeptide-1 and palmitoyl tetrapeptide-7 (sold together as Matrixyl 3000) have genuine controlled-trial support behind them. Epithalon gets a lot of attention for its telomere story, but most of that evidence still comes from animal models. Nothing on this list is a clear winner across every category at once.
Are peptides for anti-aging safe to use?
Topical peptides sold in regulated cosmetics are generally considered low-risk, since absorption through intact skin is limited. Injectable peptides are an entirely different conversation. Purity, dosing, and sourcing matter enormously, and most injectable peptides live in a legal gray zone when sold as research chemicals, with no manufacturing oversight attached to them. Anyone weighing an injectable is better off going through a physician-supervised compounding pharmacy route, like FormBlends, than buying from an unregulated online vendor.
Where should you actually buy anti-aging peptides?
For topical peptides, a reputable skincare brand with a published formulation is the safest starting point, plainly. For anything injectable, don’t buy from a research-chemical site, full stop. The absence of third-party testing and batch consistency at those vendors is a real, documented problem, not a hypothetical one. A board-certified physician or dermatologist who can order through a licensed compounding pharmacy is the only accountable path if you want to go beyond what’s already in your moisturizer.
References
- Yi L, Maier AB, Tao R, et al. The efficacy and safety of beta-nicotinamide mononucleotide (NMN) supplementation in healthy middle-aged adults: a randomized, multicenter, double-blind, placebo-controlled, parallel-group, dose-dependent clinical trial. GeroScience. 2023;45(1):29-43. doi:10.1007/s11357-022-00705-1. PMID 36482258. https://pubmed.ncbi.nlm.nih.gov/36482258/
- Diao Z, Yan Q, Zhang H, et al. The therapeutic perspective of NAD+ precursors in age-related diseases. Biochemical and Biophysical Research Communications. 2024;702:149620. doi:10.1016/j.bbrc.2024.149620. https://www.sciencedirect.com/science/article/pii/S0006291X24001256
- Khavinson VK, Morozov VG. Peptides of pineal gland and thymus prolong human life. Neuro Endocrinology Letters. 2003;24(3-4):233-240. PMID 14523363.
- Karaa A, Bertini E, Carelli V, et al. Efficacy and safety of elamipretide in individuals with primary mitochondrial myopathy: the MMPOWER-3 randomized clinical trial. Neurology. 2023;101(3):e238-e252. doi:10.1212/WNL.0000000000207402.
- Karaa A, Klopstock T, Vissing J, et al. Genotype-specific effects of elamipretide in patients with primary mitochondrial myopathy: a post hoc analysis of the MMPOWER-3 trial. Orphanet Journal of Rare Diseases. 2024;19(1):432. doi:10.1186/s13023-024-03421-5.
- Yen K, Mehta HH, Kim SJ, et al. The mitochondrial derived peptide humanin is a regulator of lifespan and healthspan. Aging (Albany NY). 2020;12(12):11185-11199. doi:10.18632/aging.103534.
- Pickart L, Margolina A. Regenerative and protective actions of the GHK-Cu peptide in the light of the new gene data. International Journal of Molecular Sciences. 2018;19(7):1987. doi:10.3390/ijms19071987. PMID 29986520.
- Liu D, Yu W, Li C, et al. The efficacy and safety of thymosin alpha 1 for sepsis (TESTS): multicentre, double blinded, randomised, placebo controlled, phase 3 trial. BMJ. 2025;388:e082583. doi:10.1136/bmj-2024-082583. PMID 39814420.
- U.S. Food and Drug Administration. FDA warns 30 telehealth companies against illegal marketing of compounded GLP-1s. March 3, 2026.
- U.S. Food and Drug Administration. Warning Letter: Prime Sciences (MARCS-CMS 721805). March 31, 2026.
Written by Finn Zamora, clinical-topics writer. Last reviewed February 2026.
Shared for informational purposes. A licensed clinician should review your plan before you start.




